FACTORS DETERMINING TAKING
REASONABLE ECONOMIC DECISIONS IN THE NON-MATERIAL SPHERE
Strzelecka A. (WZ PCz, c. Czestochowa, Poland)
Financial outlays incurred for
health care, forms of management in this sphere of national economy,
organizational systems, and economic development are considered essential when
drawing up, among other things, health programs.
Therefore the aim of this thesis is
to present the development of the factors mentioned above in selected European
countries.
Факторы, определяющие принятие разумных экономических решений в нематериальной сфере.
Introduction
The production in the considered
field of national economics is understood as provision of services that enables
execution of registered as well as potential health services. Production in the
sphere of health care is closely related to consumption of medical services
that determines the scope and size of provision of services in this sector[1].
The functioning of market mechanisms
is in large measure connected with the organizational system of health care,
forms of management of this non-material sphere, the amount of gross domestic
product, which reflects the economic potential of a country, and public
expenditure allotted for health care in a given country. Moreover, the number
of beds in hospitals and human resources, represented by the number of general
practitioners in health care, may also be recognized as factors of supply. The
share of the overall number of physicians in the overall number of population
represents payment expenses, whereas the number of beds in hospitals per capita
illustrates non-payment expenses.
For the sake of this article, the
study covered 7 European Union countries, representing different health care
systems:
The used annual statistical data
come from OECD Health Data 2004 database and include the years from 1999 to
2002[2]. Both the amount of
expenditure on health care or the amount of GDP is given in USD per
inhabitant according to the purchasing power parity.
Health care systems
1. the insurance
model, i.e. the
a)
health services are financed through
compulsory fees, which are paid by an employee as well as by an employer (or by
way of an extra tax) to a defined statutory fund;
b)
statutory funds are controlled by
self-government institutions (non-state owned) and are legal entities;
c)
funds make contributions to hospitals
(global budget);
d)
private practitioners are paid for a
service (fee-for-service);
e)
lekarze prywatni sđ
wynagradzania za usģugę (honorarium za wiadczenia);
f)
co-payment for most services;
g)
the choice of a service provider,
without a gate-keeper[3].
The countries, which
use this financial system, are e.g.
2. the budgetary model
the so-called Beveridge model:
a)
health services are financed by general
taxes;
b)
the state exercises control over
execution of services by health service a high degree of centralization;
c)
hospitals receive the global budget or
limits of financial resources divided into articles;
d)
little share of the private sector;
e)
free access to services for all citizens
is guaranteed;
f)
the gatekeeper function, regulated
access to the successive levels of care;
g)
management secured by government functionaries
guided by the general good;
h)
physicians paid by means of a salary or
capitation;
i)
patients own share in cost participation is
little.
The countries using
this health care model, among other things, are
Changes in economy of many countries also
concern the sphere of health care and through verification of already existing
solutions they are to contribute to improvement of current health policy in a
given country. As a result of these reforms, system including
the elements of both models mentioned above, i.e. the
A system that may be called a
budgetary-insurance system, as it combines features of the insurance and budgetary
system, was introduced in
The above-mentioned features determine the
current shape of health care in separate countries in which the possibly common
access to the possibly largest scope of services and financial protection of
patients always is a priority.
Forms of management in health care
Healthcare system functioning in a
given country, and especially its organization, has a large influence on
generation of health costs. Generally speaking, there are three types of
relations among funds and healthcare providers in health care models
functioning in various countries (table 1), namely:
a)
reimbursement system
b)
contract system
c)
integrated system
Table
1- Forms of management in health care in the analyzed EU countries
|
Country |
Forms of management |
|
France |
reimbursement system |
|
The |
contract system |
|
|
integrated system |
Source: Own
analysis based on Strzelecka A., (2005), p. 274.
In the reimbursement system
suppliers receive payment for delivered services on the basis of retrospectiveness. The system is often combined with
a form of direct payment for services, i.e. a system based on fee-for-service
practice.
Contract needs cooperation between
the third-party payer (the insurer) and health care suppliers, who strive to
exercise larger control over general funds and their distribution.
In integrated systems the same organizations
have control over various funds and health care suppliers. Medical personnel
are generally paid by means of a salary and budgets are, above all, an
instrument regulating health care resources.
Issues raised when analyzing health
care are directly related to the medical environment, i.e. to the influence of
the ways of paying physicians in clinic care and the increase in the number of
high-ranking medical personnel on the expenditures.
Demand created by a supplier may
arise because of several reasons although the form of delivery may be
determined and its scope depends on institutional decisions. In
the fee-for-service system physicians may regulate (adjust) their work in
response to changes in the environment in such a way that their income is
shaped at least at the same level. When demand for physicians declines
and workload lessens, physicians may persuade patients to use a larger amount
of more expensive medical services, i.e. according to the income hypothesis
there appears demand induced by supply.
Bigger competition among physicians
may encourage them to deeper engagement in their work. Physicians may work out
a treatment plan together with patients in such a way that health care services
are provided for patients in a most favorable way, even when the cost of
performed services is covered by insurance.
Moreover, predicting higher costs
connected with employing additional physicians and not creating demand may also
be accordant with classical microeconomics. Some connections between the number
of physicians and home visits may reflect real factors creating demand, e.g.
larger number of physicians may increase availability of offered health
services through reducing the distance between patients place of residence and
physicians workplace, or shortening the time of anticipation for a medical
appointment, although unit prices for an appointment are not lower as they are
administratively determined and are shaped at a constant level[4].
To conclude the above discussion, it
should be added that increasing health insurance might influence costs in
health care, by means of increase in demand as well as in supply for health
care.
Gross Domestic Product and public expenditures
on health care
The amount of investment outlays
earmarked in the Gross Domestic Product for health care is a determinant of
activities undertaken in this field of economy and of the allocation of
financial resources for health care.
Apart from the insurance system
existing in a given country, the health care expenditures are also influenced
by the value of goods and services produced in the territory of the country.
Table 2- Gross Domestic Product in
EU countries from 1999 to 2002 (in USD per capita, PPP, constant
prices)
|
System of financing health care |
Country |
Years |
Amount of GDP |
|
Insurance model |
France |
1999 |
21 850,2 |
|
2000 |
22 345,8 |
||
|
2001 |
23 147,0 |
||
|
2002 |
23 372,1 |
||
|
The |
1999 |
21 084,9 |
|
|
2000 |
21 625,0 |
||
|
2001 |
22 039,3 |
||
|
2002 |
22 204,5 |
||
|
Germany |
1999 |
19 989,0 |
|
|
2000 |
20 281,5 |
||
|
2001 |
20 081,0 |
||
|
2002 |
19 908,0 |
||
|
Insurance-budgetary model |
|
1999 |
1 808,6 |
|
2000 |
1 715,5 |
||
|
2001 |
1 680,6 |
||
|
2002 |
1 536,1 |
||
|
Budgetary model |
|
1999 |
23 032,8 |
|
2000 |
23 323,3 |
||
|
2001 |
23 725,7 |
||
|
2002 |
23 601,0 |
||
|
|
1999 |
21 650,3 |
|
|
2000 |
22 695,7 |
||
|
2001 |
22 306,9 |
||
|
2002 |
21 952,9 |
||
|
|
1999 |
19 390,3 |
|
|
2000 |
19 751,4 |
||
|
2001 |
20 474,6 |
||
|
2002 |
22 454,9 |
Source: Own study.
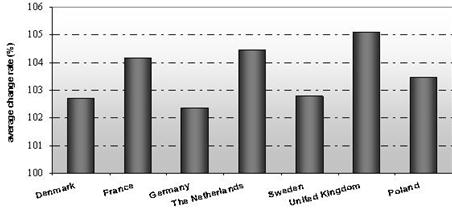
In the presented European Union countries GDP
increased on average by 3,6% year by year in the years
from 1999 to 2002. The highest increase of this measure took place at the end
of 1999 and the beginning of 2000 (it amounted to about 4,7%).
In 2002 GDP also rose, but the rate was considerably lower (2% - GDP expressed
in USD per capita). In all studied years the increase in GDP was lower
than the average rate of changes in gross domestic product for the studied EU
countries only in
While in
Table 3- Changes in levels of GDP in selected EU
countries from 1999 to 2002 (in USD per capita, PPP, current prices, previous
year =100)
|
Countries |
2000 |
2001 |
2002 |
|
previous year = 100 |
|||
|
|
104,3 |
103,8 |
100,1 |
|
|
104,3 |
105,7 |
102,6 |
|
|
103,5 |
102,0 |
101,6 |
|
The |
105,6 |
107,0 |
100,8 |
|
|
105,9 |
101,2 |
101,3 |
|
|
104,9 |
105,7 |
104,6 |
|
|
104,3 |
102,9 |
103,2 |
Sources: Own calculations on the
basis of OECD Health Data 2004.
Table4 -Changes in levels of GDP in selected EU
countries from 1999 to 2002 (in USD per capita, PPP, current prices, 1999=100)
|
Countries |
2000 |
2001 |
2002 |
|
1999 = 100 |
|||
|
Denmark |
104,3 |
108,2 |
108,3 |
|
France |
104,3 |
110,2 |
113,0 |
|
Germany |
103,5 |
105,5 |
107,2 |
|
The Netherlands |
105,6 |
113,0 |
113,9 |
|
Sweden |
105,9 |
107,2 |
108,6 |
|
United Kingdom |
104,9 |
110,9 |
116,1 |
|
Poland |
104,3 |
107,3 |
110,7 |
Sources: Own calculations on the
basis of OECD Health Data 2004.
On the
basis of this above table the average annual rate of changes in the GDP was
determined in the years 1999-2002 according the following formula:
where: y
the level of the phenomenon in the period t, t=1
n, G geometric mean
In the
years 1999-2002 the GDP in
In the remaining
countries GDP was increasing most year by year in the studied period in
Sources: Own
calculations on the basis of OECD Health Data 2004.
Figure 1- Changes in the development
of the amount of GDP in selected EU countries from 1999 to 2002 (in percents , current prices - USD per capita, PPP)
The increase in GDP
results in the increase in public expenditures on health care in almost all
analyzed countries the
Sources: Own
calculations on the basis of OECD Health Data 2004.
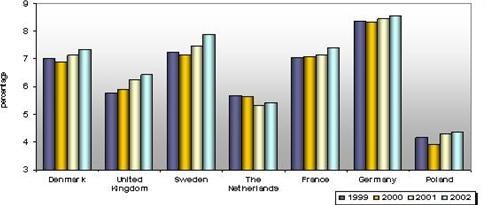
Figure 2- The share of public
expenditures on health care in GDP percent in selected EU countries from 1999
to 2000
The increase in
affluence of societies, higher level of education and awareness of citizens cause that health care services consumption is
becoming more and more important. As a general rule, private health service
units offer higher standard and wider scope of services to their patients. The
increase in public expenditures on health care is also connected with negative
birth rate. As society is getting older, the share of elderly people in the
overall number of people is increasing, which causes that health services
consumption is rising[5].
Sources: Own
calculations on the basis of OECD Health Data 2004.
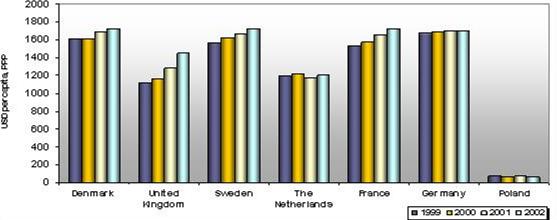
Figure 3- The development of public
expenditures on health care in selected EU countries from 1999 to 2002 (in USD
per capita, PPP, constant prices)
One the basis of the performed
analyses it may be concluded that public expenditures on health care experience
an increase in comparison with the directly preceding period but the rate of
increase decreases.
On the basis of the presented
studies of the development of expenses for health care it may be stated that in
all countries the average yearly studied amounts were growing.
Conclusion
Using health care is a very
complicated process that depends on many factors such as, among other things,
the amount of financial resources allotted for health care, forms of health
care management or organizational systems functioning in this non-material
sphere.
On the basis of analyses presented
in this thesis it may be stated that presentation of the development of public
expenditures on health care in selected European Union countries allows one to
spot some tendencies in the development of the analyzed economic quantities
over the years 1999-2002.
The performed analysis proves the
thesis that economic growth in a given country and health care system existing in it play an enormous role in the
development of public expenditures on health care. The size of the GDP
determines not only the wealth of the society but also the amount of
expenditures for health care and especially their part which is allocated by a
given country for health care.
1.
Carlsen F., Grytten
J., (1998); More physicians: improved
availability or induced demand, Health Economics 7;
2. Gerdtham U.-G., Jönsson
J., MacFarlan M., Oxley H., (1998); The
determinants of health expenditure in the OECD countries, [w:] Health, The
Medical Profession, and Regulation, red. Zweifel P., Kluwer Academic Publishes, Dordrecht;
3.
Golinowska S., (2003); Wielkoæ
i determinanty wydatków na ochronę zdrowia,
Zeszyty Naukowe Ochrony Zdrowia. Zdrowie Publiczne i Zarzđdzanie, tom I, nr 1, Kraków;
4.
OECD Health Data 2004,
(2004); A comparative analysis of 30 countries, OECD, Paris;
5. Strzelecka A., (2005); Mechanizmy
finansowania wiadczeņ zdrowotnych a formy zarzđdzania w ochronie zdrowia,
[w:] Sterowanie kosztami w zakģadach opieki zdrowotnej, red. Hass-Symotiuk M.,
PRINT GROUP Daniel Krzanowski, Szczecin;
6. Suchecka J., (1992); Modelowanie sfery
ochrony zdrowia. Problemy i metody, Wydawnictwo Uniwersytetu Ģódzkiego,
Ģód.
[1]. Suchecka J., Modelowanie sfery ochrony zdrowia. Problemy
i metody, Wydawnictwo Uniwersytetu Ģódzkiego, Ģód 1992, p. 6
[2]. 2002 is the
last year for which there is information about development of public
expenditure on health care, GDP or the number of medical practitioners in OECD
Health Data 2004.
[3]. A gatekeeper is a family
doctor who issues referrals to specialists and supervises execution of all
services to a patient registered in their practice.
[4]. Carlsen F., Grytten J., More
physicians: improved availability or induced demand, Health Economics 7,
1998, p. 495-313.
[5]. More
information connected with the influence of elderly people on the development
of expenses for health care can be found in the work by S. Golinowska
Wielkoæ i determinanty wydatków na ochronę
zdrowia, Zeszyty Naukowe Ochrony Zdrowia. Zdrowie Publiczne i Zarzđdzanie, vol. 1, Kraków 2003, p.11